
Sunday, February 27, 2011
Saturday, February 19, 2011
Goin' Down to "Pink Town"!
******
Thursday, February 17, 2011 -Pink Town
A recent article in the local newspaper caught my eye; "Fair Haven to Become 'Pink Haven' in April." This year three of my neighboring towns will be taking part in a campaign known as "Paint The Town Pink". Red Bank, Monmouth Beach and Fairhaven, will all magically morph into Pink Bank, Pink Beach and Pink Haven. All in aid of, you got it....not research...but breast cancer awareness, prevention and promotion of annual mammography for women.
Most of my regular readers will understand when I say that my first reaction to this news was to emigrate. Somewhere far away. Like Mongolia. Or Siberia. Even Antarctica seems like an attractive option. But would these places be far enough? Perhaps I can find a spot on an upcoming space mission.
The pink festival will run from April 30 through May 7. In addition to certain town roads having a pink stripe painted down the middle of them, options for community involvement include:
"...placing a pink piggy bank in a business for donations, window painting contests, pledge contests, or hosting an in-store event during the week.
Residents could also participate through a "Pink Your House" contest where residents would be provided a "Pink Starter Kit" containing lawn signs, flags, and other decorations."
Yes ! Pink your town! Pink your roads! Pink your business! Pink your house! Show your community that you don't give a crap about other cancers, or other incurable diseases, or anyone else for that matter who might not feel comfortable with all this pinkification.
Then I thought, perhaps it's time I stopped being a snarky cynic. Maybe it's time to get on board with the breast cancer celebrations and really throw myself into supporting the towns' efforts in raising funds for more breast cancer awareness. Okay, so awareness won't ever result in a cure but let's not worry about such trifling matters for now. [link to Cancer Chronicles from my profile page to read more...]
Below is an excerpt of a posting on a blog I follow: The Cancer Chronicles." I truly relate to not only the author's (Anna) writing style, but her message as well. Anna is one of those virtual voices that make feel less alone as I navigate the multiple planes of incongruity that color the lucrative cancer industry. A putrid color of bubble-gum pink. I have also included my comment to her posting at the end.

Thursday, February 17, 2011 -Pink Town
A recent article in the local newspaper caught my eye; "Fair Haven to Become 'Pink Haven' in April." This year three of my neighboring towns will be taking part in a campaign known as "Paint The Town Pink". Red Bank, Monmouth Beach and Fairhaven, will all magically morph into Pink Bank, Pink Beach and Pink Haven. All in aid of, you got it....not research...but breast cancer awareness, prevention and promotion of annual mammography for women.
Most of my regular readers will understand when I say that my first reaction to this news was to emigrate. Somewhere far away. Like Mongolia. Or Siberia. Even Antarctica seems like an attractive option. But would these places be far enough? Perhaps I can find a spot on an upcoming space mission.
The pink festival will run from April 30 through May 7. In addition to certain town roads having a pink stripe painted down the middle of them, options for community involvement include:
"...placing a pink piggy bank in a business for donations, window painting contests, pledge contests, or hosting an in-store event during the week.
Residents could also participate through a "Pink Your House" contest where residents would be provided a "Pink Starter Kit" containing lawn signs, flags, and other decorations."
Yes ! Pink your town! Pink your roads! Pink your business! Pink your house! Show your community that you don't give a crap about other cancers, or other incurable diseases, or anyone else for that matter who might not feel comfortable with all this pinkification.
Then I thought, perhaps it's time I stopped being a snarky cynic. Maybe it's time to get on board with the breast cancer celebrations and really throw myself into supporting the towns' efforts in raising funds for more breast cancer awareness. Okay, so awareness won't ever result in a cure but let's not worry about such trifling matters for now. [link to Cancer Chronicles from my profile page to read more...]
Anna - I am puking pink right now, just from reading what "Pink Haven" has in store. The irony is that all this "pink waving" campaign of awareness is exploitation and ignorance. Exploitation on the part of the orgs, companies, and retailers that turn a profit from the merchandising; and ignorance on the part of well-meaning individuals who join the pink fray without asking the key questions:
* WHOSE CAUSE IS THIS TRULY SERVING?
* HOW IS AWARENESS OF A WELL-KNOWN AND INCREASINGLY PREVALENT DISEASE TRANSLATING INTO TANGIBLE STEPS TOWARD FINDING A CURE?
* WHY, DESPITE THE ONGOING PINK PARADES, ARE MORE WOMEN BEING AFFECTED BY BREAST CANCER?
* WHY IS BREAST CANCER SUCH A LUCRATIVE NICHE INDUSTRY?
* WHY IS IT THAT THE SAME COMPANIES THAT FUND TRIALS FOR "NEW CURES" SIMULTANEOUSLY PRODUCE PRODUCTS WITH KNOWN CARCINOGENS? I could go on, but I think I made my point. Anna, I applaud you fighting the "Pink Beast" in whichever way you can/choose. I believe that the Pink Beast truly does more harm, has a palpable chilling effect on a real discussion, and detrimentally distracts people from asking the truly critical questions about the epidemic of breast cancer.

Wednesday, February 16, 2011
Hot Flashes Linked to Lower Breast Cancer Risk...Hmmm, Maybe
******
Study Suggests Hot Flashes in Menopause May Reduce Risk of 2 Types of Breast Cancer
 By Brenda Goodman
By Brenda Goodman
WebMD Health News
Reviewed by Laura J. Martin, MD
Jan. 28, 2011
A new study shows that having symptoms such as hot flashes during menopause appears to be tied to a lower risk of the most common kinds of breast cancer.
“There’s good news about hot flashes,” says Susan Love, MD, a breast cancer expert and author of Dr. Susan Love’s Menopause and Hormone Book.
Researchers from the Fred Hutchinson Cancer Center in Seattle interviewed more than 1,000 women with one of three kinds of breast cancer and compared them to nearly 500 randomly selected women of similar ages with no history of breast cancer.
Participants were asked whether they ever experienced menopausal symptoms, including hot flashes, sweating or night sweats, vaginal dryness, bladder problems, irregular or heavy menstrual bleeding, depression, anxiety, insomnia, or emotional distress.
With regard to hot flashes, women were asked how often they occurred, how long they typically lasted, and for how many total weeks or months they had them.
Compared to women who reported never having menopausal symptoms, those who had experienced symptoms had half the risk of invasive ductal carcinoma or invasive lobular carcinoma, two of the most common types of breast cancer.
And the more frequent or severe the hot flashes were, the lower their risk appeared to be.
Those associations remained even after researchers took into account other things that are known to influence breast cancer risk, such as the use of hormone replacement therapy, age at menopause, and body weight.
The study is published in the February issue of Cancer Epidemiology, Biomarkers & Prevention.
"This is the first study to ever look at this association,” says study researcher Christopher I. Li, MD, PhD, a breast cancer epidemiologist in the Hutchinson Center’s Public Health Sciences Division.
Li stresses, however, that his study was not designed to show cause and effect, and that the connection between menopausal symptoms and breast cancer is still largely a mystery.
“We don’t know a whole lot about all the biology that’s at work here,” he says.
In particular, scientists don’t know what causes hot flashes, only that they appear to be linked to lower levels of the hormone estrogen.
Breast cancer, in turn, has been linked to higher levels of estrogen, so it may be that hot flashes are acting as a marker for the intensity of hormonal changes in the body, Li says.
Indeed, a previous study showed that women who experienced hot flashes several times a day had 35% to 45% lower estrogen levels compared with women who did not experience hot flashes or who only experienced them infrequently.
Rush Hour Thinking....The following reprinted article came from one of the institutional e-newsletters I receive. I initially read it off of my Blackberry while sitting in wall-to-wall traffic on a highway. (And no, the car was not moving, I assure you. But it sure got my mind moving in wild directions.) I know that these snip-its don't provide a reader with the whole back-story. I do plan to scrutinize the original publication. I must say, however, upon reading this I felt like I had been punched in the gut. It highlighted a conundrum for me. Specifically, the incongruity of breast cancer in pre-menopausal women.
I was not menopausal when I discovered the cancer growing within me. I have no experience with hot flashes. That said, my last cycle was three months ago. Since my bout with pneumonia in December, nothing is working properly. Is this menopause? I have no other telling symptoms. Is it amenoria? Possibly. It has happened to me before - but I was a lot younger. If this is actually "symptom-free" menopause, then the below snip-it truly may be on to something.
The other punch that this article laid on me was the paradox between estrogen levels and breast cancer. My form of cancer, invasive lobular carcinoma (ILC), has been determined to be an estrogen-driven form of breast cancer. It has been hypothesized that my body does not eliminate estrogen properly. As a result, a build up of estrogen in my body became toxic / carcinogenic, and voila -- a fertile environment for cancer to grow. It would then appear, based on this theory, that my body "naturally" stores (or stored) a high level of estrogen. The below snip-it reports that hot flashes are believed to be the result of low estrogen levels in the body. I am not experiencing anything resembling a "hot flash." It would appear, then, that my own experience may support the theory.
I then took the leap to connect the dots in uncovering the "truth" about my own development of breast cancer. I started to rethink my history of multiple miscarriages. With each miscarriage it appeared that my hCG levels were not high enough to sustain the pregnancy. To my knowledge, there is no definitive evidence linking miscarriages and breast cancer. That said, there are clinical trials [See, Science Daily (Apr. 25, 2009) & Fox Chase Cancer Center] testing the use of hCG (human chorionic gonadotropin) as an anti-cancer agent. The study is based on the thought that full term pregnancies earlier in a woman's life is a potential prophylactic against the development of breast cancer later in life. Recall, estrogen are steroids. They play a large role in a woman's monthly cycle, as well as in a pregnancy.
This then brought me to further bridge the chasm and consider the potential of a causal relationship between my reproductive hx of multiple miscarriages and low hCG levels (if hCG in indeed an anti-cancer agent), my lack of menopausal symptoms (theorized to be an indicator of high estrogen levels), and the development of ILC (an estrogen driven form of breast cancer). It is amazing the tangents the mind can indulge in when stuck in rush-hour traffic. Just proves the adage...a little knowledge can be a very dangerous thing.

Study Suggests Hot Flashes in Menopause May Reduce Risk of 2 Types of Breast Cancer

WebMD Health News
Reviewed by Laura J. Martin, MD
Jan. 28, 2011
A new study shows that having symptoms such as hot flashes during menopause appears to be tied to a lower risk of the most common kinds of breast cancer.
“There’s good news about hot flashes,” says Susan Love, MD, a breast cancer expert and author of Dr. Susan Love’s Menopause and Hormone Book.
Researchers from the Fred Hutchinson Cancer Center in Seattle interviewed more than 1,000 women with one of three kinds of breast cancer and compared them to nearly 500 randomly selected women of similar ages with no history of breast cancer.
Participants were asked whether they ever experienced menopausal symptoms, including hot flashes, sweating or night sweats, vaginal dryness, bladder problems, irregular or heavy menstrual bleeding, depression, anxiety, insomnia, or emotional distress.
With regard to hot flashes, women were asked how often they occurred, how long they typically lasted, and for how many total weeks or months they had them.
Compared to women who reported never having menopausal symptoms, those who had experienced symptoms had half the risk of invasive ductal carcinoma or invasive lobular carcinoma, two of the most common types of breast cancer.
And the more frequent or severe the hot flashes were, the lower their risk appeared to be.
Those associations remained even after researchers took into account other things that are known to influence breast cancer risk, such as the use of hormone replacement therapy, age at menopause, and body weight.
The study is published in the February issue of Cancer Epidemiology, Biomarkers & Prevention.
"This is the first study to ever look at this association,” says study researcher Christopher I. Li, MD, PhD, a breast cancer epidemiologist in the Hutchinson Center’s Public Health Sciences Division.
Li stresses, however, that his study was not designed to show cause and effect, and that the connection between menopausal symptoms and breast cancer is still largely a mystery.
“We don’t know a whole lot about all the biology that’s at work here,” he says.
In particular, scientists don’t know what causes hot flashes, only that they appear to be linked to lower levels of the hormone estrogen.
Breast cancer, in turn, has been linked to higher levels of estrogen, so it may be that hot flashes are acting as a marker for the intensity of hormonal changes in the body, Li says.
Indeed, a previous study showed that women who experienced hot flashes several times a day had 35% to 45% lower estrogen levels compared with women who did not experience hot flashes or who only experienced them infrequently.
Friday, February 11, 2011
Voices
******


I will become truly worried when the little voices cut out the middle-person and start talking directly to each other.
Thursday, February 10, 2011
A little whining.
******
I have not whined in awhile. Ranted, yes. Personally played my own pity violin - not in awhile. I am due.
 I find that I am tired. Almost all of the time.
I find that I am tired. Almost all of the time.
I have noticed that the dark blue circles under my eyes are becoming fixtures, and creeping slowly toward where the "apples" of my cheeks used to be. I am going through the concealer like its lip balm.
At times I sleep, literally, like the dead. Other times, the slightest sound, rustle, movement startles me awake.
The dreams are curiouser and curiouser.
The pains are curiouser and curiouser; and more persistent.
My body feels like its on full-tilt. I am so keenly aware of every breath, every rumble, every stab, stress, pull, pop. Yet, at the same time I am disassociated from it all.
Something new will manifest, and take hold. My husband asks: "are you concerned?"
Sometimes.
The little voice buried in my semi-conscious wonders "is this symptomatic of ...?..." "should I pull out the latest written orders for tests and just allow the poking and prodding to go on?" "Do you really want to do a fourth vaginal ultrasound and pelvic MRI, just because no one can definitively determine what that pesky little pain & mass are?"
I do pull out the orders that are in my vanity drawer (how's that for irony) look them over, and stuff them back inside. They have been in the drawer since January now.
My other little voice then loudly pronounces, "what would you do if they can figure it all out?" And the resounding response is, "probably nothing that they would find acceptable."
 So, unless they can make a vaginal ultrasound fun -- and I am talking fun like they are able to get Johnny Depp to hold the wand, then NO, I don't want to go through it again for a fourth time in 10 months.
So, unless they can make a vaginal ultrasound fun -- and I am talking fun like they are able to get Johnny Depp to hold the wand, then NO, I don't want to go through it again for a fourth time in 10 months.
...
And, at the same time I am doing all this wild body-morphing activities (hot yoga, reiki-ish realignments, colonic therapy, infra-red saunas...elixirs and tonics). Still, I feel drained, spent and unmotivated. Interestingly, not when I am in the middle of an experience. Before, after.
It's life after cancer? It's life with cancer? It's life pushing 50?
I have noticed that the dark blue circles under my eyes are becoming fixtures, and creeping slowly toward where the "apples" of my cheeks used to be. I am going through the concealer like its lip balm.
At times I sleep, literally, like the dead. Other times, the slightest sound, rustle, movement startles me awake.
The dreams are curiouser and curiouser.
The pains are curiouser and curiouser; and more persistent.
My body feels like its on full-tilt. I am so keenly aware of every breath, every rumble, every stab, stress, pull, pop. Yet, at the same time I am disassociated from it all.
Something new will manifest, and take hold. My husband asks: "are you concerned?"
Sometimes.
The little voice buried in my semi-conscious wonders "is this symptomatic of ...?..." "should I pull out the latest written orders for tests and just allow the poking and prodding to go on?" "Do you really want to do a fourth vaginal ultrasound and pelvic MRI, just because no one can definitively determine what that pesky little pain & mass are?"
I do pull out the orders that are in my vanity drawer (how's that for irony) look them over, and stuff them back inside. They have been in the drawer since January now.
My other little voice then loudly pronounces, "what would you do if they can figure it all out?" And the resounding response is, "probably nothing that they would find acceptable."

...
And, at the same time I am doing all this wild body-morphing activities (hot yoga, reiki-ish realignments, colonic therapy, infra-red saunas...elixirs and tonics). Still, I feel drained, spent and unmotivated. Interestingly, not when I am in the middle of an experience. Before, after.
It's life after cancer? It's life with cancer? It's life pushing 50?
Wednesday, February 9, 2011
Sentinel Node Biopsies (SNB)...Unnecessary?
******
Lymph Node Study Shakes Pillar of Breast Cancer Care
By DENISE GRADY (February 8, 2011 - NY Times)
A new study finds that many women with early breast cancer do not need a painful procedure that has long been routine: removal of cancerous lymph nodes from the armpit.
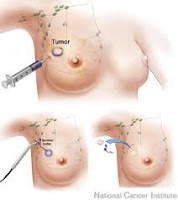
Part and parcel of my mastectomy back in August 2009 included what is termed: a sentinel node biopsy (SNB). This is where, as a matter of protocol, the surgical oncologist removes the first few nodes from the armpit, closest in proximity of the cancerous tumor. This is surgically accomplished after a lengthy prep of injecting the nodes - through the breast tissue, with radioactive material. The trick is then to keep the patient (moi) still for nearly an hour's time, to allow the radioactive material to settle into the nodes. It is this "settling" that gives the surgeon direction as to which nodes to remove. Once removed, and while the mastectomy is concurrently being done, a pathologist reviews these nodes and determines if any further excision is required.
The discovery turns standard medical practice on its head. Surgeons have been removing lymph nodes from under the arms of breast cancer patients for 100 years, believing it would prolong women’s lives by keeping the cancer from spreading or coming back.
One would think that after 100 years of post-surgical study that this "new" information / possibility / probability should have, could have been discovered / explored sooner. The latency of this revelation, in and of itself, is greatly disturbing. And there is the tiny little fact that DESPITE having had a SNB; and DESPITE the fact that I did have one positive node but current medical protocol was to ignore it as a "false positive" -- attributable to the SNB itself...nearly two (2) years to the day it is confirmed that my breast cancer has indeed spread into my lymphatic system. What does this mean? Well, because of the active lymph nodes being so close to the primary tumor site, there is a very high probability that distant organs are affected. The challenge with ILC is, however, that it is difficult to early detect any potentially affected organ because until the invasive forms into a detectable mass. Which is my cancer hx thus far.
Now, researchers report that for women who meet certain criteria — about 20 percent of patients, or 40,000 women a year in the United States — taking out cancerous nodes has no advantage. It does not change the treatment plan, improve survival or make the cancer less likely to recur. And it can cause complications like infection and lymphedema, a chronic swelling in the arm that ranges from mild to disabling.
I was very fortunate. Aside from some initial post-surgical swelling, I did not develop lymphedema -- although my med-pro team was fully anticipating I would. Because of the SNB, however, I need to ensure that during any sort of medical examination (routine or otherwise) my blood pressure is not taken on my left side -- the SNB site. Reason: lymphedema can occur at any time by this simple routine exam as a result of having had an SNB. It is notable that even when I am being examined by a member of my "cancer team" I still have to remind each and every one of them -- each and every time, not to measure my blood pressure on my left-side. Inevitably, and strangely, they all gravitate to the left.
Removing the cancerous lymph nodes proved unnecessary because the women in the study had chemotherapy and radiation, which probably wiped out any disease in the nodes, the researchers said. Those treatments are now standard for women with breast cancer in the lymph nodes, based on the realization that once the disease reaches the nodes, it has the potential to spread to vital organs and cannot be eliminated by surgery alone.
 This aspect of the study particularly interests me for two reasons: (1) One of out of the three nodes that I had removed did test positive for cancer cells. I was told, however, that because of a then-recent study in 2009, protocol had changed and advised that there was a strong probability that cancer cells are unintentionally injected into the nodes as a result of the surgical procedure itself. As such, since it was my third node that was positive, the "protocol" was "to do nothing" further, surgically. (2) That said, anyone following my journey will know that I opted out of both chemo and radiation -- despite the heavy-handed pressure by my "cancer team" to aggressively pursue both. I opted out, because of: (a) the disparity within the global medical community as to the efficacy of chemo and radiation in prolonging life after cancer; (b) my own personal "efficacy" test (Oncotype DX) that concluded I would only have up to a 4% margin of efficacy if I underwent chemo; and (c) not finding one medical professional who themselves would subject themselves to radiation treatment (though none of them would "publicly" admit these personal views).
This aspect of the study particularly interests me for two reasons: (1) One of out of the three nodes that I had removed did test positive for cancer cells. I was told, however, that because of a then-recent study in 2009, protocol had changed and advised that there was a strong probability that cancer cells are unintentionally injected into the nodes as a result of the surgical procedure itself. As such, since it was my third node that was positive, the "protocol" was "to do nothing" further, surgically. (2) That said, anyone following my journey will know that I opted out of both chemo and radiation -- despite the heavy-handed pressure by my "cancer team" to aggressively pursue both. I opted out, because of: (a) the disparity within the global medical community as to the efficacy of chemo and radiation in prolonging life after cancer; (b) my own personal "efficacy" test (Oncotype DX) that concluded I would only have up to a 4% margin of efficacy if I underwent chemo; and (c) not finding one medical professional who themselves would subject themselves to radiation treatment (though none of them would "publicly" admit these personal views).
Experts say that the new findings, combined with similar ones from earlier studies, should change medical practice for many patients. Some centers have already acted on the new information. Memorial Sloan-Kettering Cancer Center in Manhattan changed its practice in September, because doctors knew the study results before they were published. But more widespread change may take time, experts say, because the belief in removing nodes is so deeply ingrained.
“This is such a radical change in thought that it’s been hard for many people to get their heads around it,” said Dr. Monica Morrow, chief of the breast service at Sloan-Kettering and an author of the study, which is being published Wednesday in The Journal of the American Medical Association. The National Cancer Institute paid for the study.
This again begs my initial question -- why did this "radical change" take 100 years to publicly disseminate.
Doctors and patients alike find it easy to accept more cancer treatment on the basis of a study, Dr. Morrow said, but get scared when the data favor less treatment.
 The above statement makes me ponder just how many of us "patients" they polled. Sadly, I find that many of my fellow breast cancer-club member's have made far-reaching medical decisions solely based on their initial fears. On the other hand, I have also found, and continue to find, a growing number of club members who share my belief that decisions can only be made after extensive research and questioning. And, after extensive research and questioning many of us discover that the "science" behind adjuvant treatment does not play out in our favor; so we opt-out.
The above statement makes me ponder just how many of us "patients" they polled. Sadly, I find that many of my fellow breast cancer-club member's have made far-reaching medical decisions solely based on their initial fears. On the other hand, I have also found, and continue to find, a growing number of club members who share my belief that decisions can only be made after extensive research and questioning. And, after extensive research and questioning many of us discover that the "science" behind adjuvant treatment does not play out in our favor; so we opt-out.
The new findings are part of a trend to move away from radical surgery for breast cancer. Rates of mastectomy, removal of the whole breast, began declining in the 1980s after studies found that for many patients, survival rates after lumpectomy and radiation were just as good as those after mastectomy.
The trend reflects an evolving understanding of breast cancer. In decades past, there was a belief that surgery could “get it all” — eradicate the cancer before it could spread to organs and bones. But research has found that breast cancer can begin to spread early, even when tumors are small, leaving microscopic traces of the disease after surgery.
To the credit of my surgical oncologist (Lise Walker) she was not so arrogant as to believe that surgery could "get it all." Indeed, she and I had a spirited discussion of the known microscopic cancer cells that were left in my body post-mastectomy. FYI - I did not have the option of a lumpectomy. My tumor was 6.2 cm - i.e., of such expanse that it spread throughout my entire left breast. BTW - it was in Lise Walker's office that I first discovered the book: "What Your Doctor Won't Tell You About Breast Cancer."
The modern approach is to cut out obvious tumors — because lumps big enough to detect may be too dense for drugs and radiation to destroy — and to use radiation and chemotherapy to wipe out microscopic disease in other places.
Modern? Cut, slash and burn has been the protocol for over 50+ years.
But doctors have continued to think that even microscopic disease in the lymph nodes should be cut out to improve the odds of survival. And until recently, they counted cancerous lymph nodes to gauge the severity of the disease and choose chemotherapy. But now the number is not so often used to determine drug treatment, doctors say. What matters more is whether the disease has reached any nodes at all. If any are positive, the disease could become deadly. Chemotherapy is recommended, and the drugs are the same, no matter how many nodes are involved.
This latter sentence is frightening. Not because it causes me to reflect on my choice not to undergo adjuvant treatment. But because it is these types of statements that were used to try and bully me into acquiescing to chemo and radiation -- despite the undisputed medical conclusion that I would not benefit from chemo. It is these types of statements that plant fear into persons dealing with breast cancer and emotionally and mentally inhibits them from becoming informed patients.
"...and the drugs are the same, no matter how many nodes are involved." This admission also sends chills down my spine. It should be a big ol' red flag that in light of it taking the med-pros 100 years to publicly declare this "nodal" revelation, that the med-pros are still unwilling, as a community, to reveal that the "standard protocol" for treating breast cancer reached a plateau decades ago. Refer back to my "audience with the Great Oz back in September, 2009."
The new results do not apply to all patients, only to women whose disease and treatment meet the criteria in the study.
 The tumors were early, at clinical stage T1 or T2, meaning less than two inches across. Biopsies of one or two armpit nodes had found cancer, but the nodes were not enlarged enough to be felt during an exam, and the cancer had not spread anywhere else. The women had lumpectomies, and most also had radiation to the entire breast, and chemotherapy or hormone-blocking drugs, or both.
The tumors were early, at clinical stage T1 or T2, meaning less than two inches across. Biopsies of one or two armpit nodes had found cancer, but the nodes were not enlarged enough to be felt during an exam, and the cancer had not spread anywhere else. The women had lumpectomies, and most also had radiation to the entire breast, and chemotherapy or hormone-blocking drugs, or both.
The study, at 115 medical centers, included 891 patients. Their median age was in the mid-50s, and they were followed for a median of 6.3 years.
After the initial node biopsy, the women were assigned at random to have 10 or more additional nodes removed, or to leave the nodes alone. In 27 percent of the women who had additional nodes removed, those nodes were cancerous. But over time, the two groups had no difference in survival: more than 90 percent survived at least five years. Recurrence rates in the armpit were also similar, less than 1 percent. If breast cancer is going to recur under the arm, it tends to do so early, so the follow-up period was long enough, the researchers said.
One potential weakness in the study is that there was not complete follow-up information on 166 women, about equal numbers from each group. The researchers said that did not affect the results. A statistician who was not part of the study said the missing information should have been discussed further, but probably did not have an important impact.
It is not known whether the findings also apply to women who do not have radiation and chemotherapy, or to those who have only part of the breast irradiated. Nor is it known whether the findings could be applied to other types of cancer.
The results mean that women like those in the study will still have to have at least one lymph node removed, to look for cancer and decide whether they will need more treatment. But taking out just one or a few nodes should be enough.
Dr. Armando E. Giuliano, the lead author of the study and the chief of surgical oncology at the John Wayne Cancer Institute at St. John’s Health Center in Santa Monica, Calif., said: “It shouldn’t come as a big surprise, but it will. It’s hard for us as surgeons and medical oncologists and radiation oncologists to accept that you don’t have to remove the nodes in the armpit.”
Dr. Grant W. Carlson, a professor of surgery at the Winship Cancer Institute at Emory University, and the author of an editorial accompanying the study, said that by routinely taking out many nodes, “I have a feeling we’ve been doing a lot of harm.”
Indeed, women in the study who had the nodes taken out were far more likely (70 percent versus 25 percent) to have complications like infections, abnormal sensations and fluid collecting in the armpit. They were also more likely to have lymphedema.
I can attest to the abnormal sensations (euphemism for pain), that continue each and every day, to this day, since the SNB and mastectomy in August 2009.
But Dr. Carlson said that some of his colleagues, even after hearing the new study results, still thought the nodes should be removed.
“The dogma is strong,” he said. “It’s a little frustrating.”
This understated sentiment can be broadly applied in all aspects of the breast cancer industry.
Eventually, he said, genetic testing of breast tumors might be enough to determine the need for treatment, and eliminate the need for many node biopsies.
Had extensive genetic testing prior to the SNB and mastectomy. Did not alter the course of treatment adamantly lobbied for by the "cancer team."
Two other breast surgeons not involved with the study said they would take it seriously.
Dr. Elisa R. Port, the chief of breast surgery at Mount Sinai Medical Center in Manhattan, said: “It’s a big deal in the world of breast cancer. It’s definitely practice-changing.”
Dr. Alison Estabrook, the chief of the comprehensive breast center at St. Luke’s-Roosevelt hospital in New York said surgeons had long been awaiting the results.
“In the past, surgeons thought our role was to get out all the cancer,” Dr. Estabrook said. “Now he’s saying we don’t really have to do that.”
But both Dr. Estabrook and Dr. Port said they would still have to make judgment calls during surgery and remove lymph nodes that looked or felt suspicious.
The new research grew out of efforts in the 1990s to minimize lymph node surgery in the armpit, called axillary dissection. Surgeons developed a technique called sentinel node biopsy, in which they injected a dye into the breast and then removed just one or a few nodes that the dye reached first, on the theory that if the tumor was spreading, cancer cells would show up in those nodes. If there was no cancer, no more nodes were taken. But if there were cancer cells, the surgeon would cut out more nodes.
Although the technique spared many women, many others with positive nodes still had extensive cutting in the armpit, and suffered from side effects.
“Women really dread the axillary dissection,” Dr. Giuliano said. “They fear lymphedema. There’s numbness, shoulder pain, and some have limitation of motion. There are a fair number of serious complications. Women know it.”
After armpit surgery, 20 percent to 30 percent of women develop lymphedema, Dr. Port said, and radiation may increase the rate to 40 percent to 50 percent. Physical therapy can help, but there is no cure.
The complications — and the fact that there was no proof that removing the nodes prolonged survival — inspired Dr. Giuliano to compare women with and without axillary dissection. Some doctors objected. They were so sure cancerous nodes had to come out that they said the study was unethical and would endanger women.
“Some prominent institutions wouldn’t even take part in it,” Dr. Giuliano said, though he declined to name them. “They’re very supportive now. We don’t want to hurt their feelings. They’ve seen the light.”
Normally when I reprint an article or study for PSA purposes I don't include, within the text, my own editorial comments. In this case, with this study, I feel compelled to throw my "two cents" in ... smack dab in the middle of the reporting. My comments, editorials, opinions, etc are noted in italics. Read on...the "dogma is strong!"
By DENISE GRADY (February 8, 2011 - NY Times)
A new study finds that many women with early breast cancer do not need a painful procedure that has long been routine: removal of cancerous lymph nodes from the armpit.
 |
| Medical diagram of SNB Prep |
The discovery turns standard medical practice on its head. Surgeons have been removing lymph nodes from under the arms of breast cancer patients for 100 years, believing it would prolong women’s lives by keeping the cancer from spreading or coming back.
One would think that after 100 years of post-surgical study that this "new" information / possibility / probability should have, could have been discovered / explored sooner. The latency of this revelation, in and of itself, is greatly disturbing. And there is the tiny little fact that DESPITE having had a SNB; and DESPITE the fact that I did have one positive node but current medical protocol was to ignore it as a "false positive" -- attributable to the SNB itself...nearly two (2) years to the day it is confirmed that my breast cancer has indeed spread into my lymphatic system. What does this mean? Well, because of the active lymph nodes being so close to the primary tumor site, there is a very high probability that distant organs are affected. The challenge with ILC is, however, that it is difficult to early detect any potentially affected organ because until the invasive forms into a detectable mass. Which is my cancer hx thus far.
Now, researchers report that for women who meet certain criteria — about 20 percent of patients, or 40,000 women a year in the United States — taking out cancerous nodes has no advantage. It does not change the treatment plan, improve survival or make the cancer less likely to recur. And it can cause complications like infection and lymphedema, a chronic swelling in the arm that ranges from mild to disabling.
 |
| Example of lymphedema patient with a medical sleeve |
Removing the cancerous lymph nodes proved unnecessary because the women in the study had chemotherapy and radiation, which probably wiped out any disease in the nodes, the researchers said. Those treatments are now standard for women with breast cancer in the lymph nodes, based on the realization that once the disease reaches the nodes, it has the potential to spread to vital organs and cannot be eliminated by surgery alone.
Experts say that the new findings, combined with similar ones from earlier studies, should change medical practice for many patients. Some centers have already acted on the new information. Memorial Sloan-Kettering Cancer Center in Manhattan changed its practice in September, because doctors knew the study results before they were published. But more widespread change may take time, experts say, because the belief in removing nodes is so deeply ingrained.
“This is such a radical change in thought that it’s been hard for many people to get their heads around it,” said Dr. Monica Morrow, chief of the breast service at Sloan-Kettering and an author of the study, which is being published Wednesday in The Journal of the American Medical Association. The National Cancer Institute paid for the study.
This again begs my initial question -- why did this "radical change" take 100 years to publicly disseminate.
Doctors and patients alike find it easy to accept more cancer treatment on the basis of a study, Dr. Morrow said, but get scared when the data favor less treatment.

The new findings are part of a trend to move away from radical surgery for breast cancer. Rates of mastectomy, removal of the whole breast, began declining in the 1980s after studies found that for many patients, survival rates after lumpectomy and radiation were just as good as those after mastectomy.
The trend reflects an evolving understanding of breast cancer. In decades past, there was a belief that surgery could “get it all” — eradicate the cancer before it could spread to organs and bones. But research has found that breast cancer can begin to spread early, even when tumors are small, leaving microscopic traces of the disease after surgery.
 |
| Sentinel node biopsy incision |
The modern approach is to cut out obvious tumors — because lumps big enough to detect may be too dense for drugs and radiation to destroy — and to use radiation and chemotherapy to wipe out microscopic disease in other places.
Modern? Cut, slash and burn has been the protocol for over 50+ years.
But doctors have continued to think that even microscopic disease in the lymph nodes should be cut out to improve the odds of survival. And until recently, they counted cancerous lymph nodes to gauge the severity of the disease and choose chemotherapy. But now the number is not so often used to determine drug treatment, doctors say. What matters more is whether the disease has reached any nodes at all. If any are positive, the disease could become deadly. Chemotherapy is recommended, and the drugs are the same, no matter how many nodes are involved.
This latter sentence is frightening. Not because it causes me to reflect on my choice not to undergo adjuvant treatment. But because it is these types of statements that were used to try and bully me into acquiescing to chemo and radiation -- despite the undisputed medical conclusion that I would not benefit from chemo. It is these types of statements that plant fear into persons dealing with breast cancer and emotionally and mentally inhibits them from becoming informed patients.
 |
| Injection of the the radioactive material in prep for the node biopsy |
"...and the drugs are the same, no matter how many nodes are involved." This admission also sends chills down my spine. It should be a big ol' red flag that in light of it taking the med-pros 100 years to publicly declare this "nodal" revelation, that the med-pros are still unwilling, as a community, to reveal that the "standard protocol" for treating breast cancer reached a plateau decades ago. Refer back to my "audience with the Great Oz back in September, 2009."
The new results do not apply to all patients, only to women whose disease and treatment meet the criteria in the study.

The study, at 115 medical centers, included 891 patients. Their median age was in the mid-50s, and they were followed for a median of 6.3 years.
After the initial node biopsy, the women were assigned at random to have 10 or more additional nodes removed, or to leave the nodes alone. In 27 percent of the women who had additional nodes removed, those nodes were cancerous. But over time, the two groups had no difference in survival: more than 90 percent survived at least five years. Recurrence rates in the armpit were also similar, less than 1 percent. If breast cancer is going to recur under the arm, it tends to do so early, so the follow-up period was long enough, the researchers said.
One potential weakness in the study is that there was not complete follow-up information on 166 women, about equal numbers from each group. The researchers said that did not affect the results. A statistician who was not part of the study said the missing information should have been discussed further, but probably did not have an important impact.
It is not known whether the findings also apply to women who do not have radiation and chemotherapy, or to those who have only part of the breast irradiated. Nor is it known whether the findings could be applied to other types of cancer.
The results mean that women like those in the study will still have to have at least one lymph node removed, to look for cancer and decide whether they will need more treatment. But taking out just one or a few nodes should be enough.
Dr. Armando E. Giuliano, the lead author of the study and the chief of surgical oncology at the John Wayne Cancer Institute at St. John’s Health Center in Santa Monica, Calif., said: “It shouldn’t come as a big surprise, but it will. It’s hard for us as surgeons and medical oncologists and radiation oncologists to accept that you don’t have to remove the nodes in the armpit.”
Dr. Grant W. Carlson, a professor of surgery at the Winship Cancer Institute at Emory University, and the author of an editorial accompanying the study, said that by routinely taking out many nodes, “I have a feeling we’ve been doing a lot of harm.”
Indeed, women in the study who had the nodes taken out were far more likely (70 percent versus 25 percent) to have complications like infections, abnormal sensations and fluid collecting in the armpit. They were also more likely to have lymphedema.
I can attest to the abnormal sensations (euphemism for pain), that continue each and every day, to this day, since the SNB and mastectomy in August 2009.
But Dr. Carlson said that some of his colleagues, even after hearing the new study results, still thought the nodes should be removed.
“The dogma is strong,” he said. “It’s a little frustrating.”
This understated sentiment can be broadly applied in all aspects of the breast cancer industry.
Eventually, he said, genetic testing of breast tumors might be enough to determine the need for treatment, and eliminate the need for many node biopsies.
 |
| BRCA Genes I & II Mutation |
Two other breast surgeons not involved with the study said they would take it seriously.
Dr. Elisa R. Port, the chief of breast surgery at Mount Sinai Medical Center in Manhattan, said: “It’s a big deal in the world of breast cancer. It’s definitely practice-changing.”
Dr. Alison Estabrook, the chief of the comprehensive breast center at St. Luke’s-Roosevelt hospital in New York said surgeons had long been awaiting the results.
“In the past, surgeons thought our role was to get out all the cancer,” Dr. Estabrook said. “Now he’s saying we don’t really have to do that.”
But both Dr. Estabrook and Dr. Port said they would still have to make judgment calls during surgery and remove lymph nodes that looked or felt suspicious.
The new research grew out of efforts in the 1990s to minimize lymph node surgery in the armpit, called axillary dissection. Surgeons developed a technique called sentinel node biopsy, in which they injected a dye into the breast and then removed just one or a few nodes that the dye reached first, on the theory that if the tumor was spreading, cancer cells would show up in those nodes. If there was no cancer, no more nodes were taken. But if there were cancer cells, the surgeon would cut out more nodes.
Although the technique spared many women, many others with positive nodes still had extensive cutting in the armpit, and suffered from side effects.
 |
| A lymphedema patient, without the medical sleeve |
After armpit surgery, 20 percent to 30 percent of women develop lymphedema, Dr. Port said, and radiation may increase the rate to 40 percent to 50 percent. Physical therapy can help, but there is no cure.
The complications — and the fact that there was no proof that removing the nodes prolonged survival — inspired Dr. Giuliano to compare women with and without axillary dissection. Some doctors objected. They were so sure cancerous nodes had to come out that they said the study was unethical and would endanger women.
“Some prominent institutions wouldn’t even take part in it,” Dr. Giuliano said, though he declined to name them. “They’re very supportive now. We don’t want to hurt their feelings. They’ve seen the light.”
Saturday, February 5, 2011
The Pill & Breast Cancer ... PSA
******
A woman’s risk of developing breast cancer depends on several factors, some of which are related to her natural hormones. Hormonal factors that increase the risk of breast cancer include conditions that may allow high levels of hormones to persist for long periods of time, such as beginning menstruation at an early age (before age 12), experiencing menopause at a late age (after age 55), having a first child after age 30, and not having children at all.
A 1996 analysis of worldwide epidemiologic data conducted by the Collaborative Group on Hormonal Factors in Breast Cancer found that women who were current or recent users of birth control pills had a slightly elevated risk of developing breast cancer. The risk was highest for women who started using OCs as teenagers. However, 10 or more years after women stopped using OCs, their risk of developing breast cancer returned to the same level as if they had never used birth control pills, regardless of family history of breast cancer, reproductive history, geographic area of residence, ethnic background, differences in study design, dose and type of hormone, or duration of use. In addition, breast cancers diagnosed in women after 10 or more years of not using OCs were less advanced than breast cancers diagnosed in women who had never used OCs. To conduct this analysis, the researchers examined the results of 54 studies. The analysis involved 53,297 women with breast cancer and 100,239 women without breast cancer. More than 200 researchers participated in this combined analysis of their original studies, which represented about 90 percent of the epidemiological studies throughout the world that had investigated the possible relationship between OCs and breast cancer (2).
The findings of the Women’s Contraceptive and Reproductive Experiences (Women’s CARE) study were in contrast to those described above. The Women’s CARE study examined the use of OCs as a risk factor for breast cancer in women ages 35 to 64. Researchers interviewed 4,575 women who were diagnosed with breast cancer between 1994 and 1998, and 4,682 women who did not have breast cancer. Investigators collected detailed information about the participants’ use of OCs, reproductive history, health, and family history. The results, which were published in 2002, indicated that current or former use of OCs did not significantly increase the risk of breast cancer. The findings were similar for white and black women. Factors such as longer periods of use, higher doses of estrogen, initiation of OC use before age 20, and OC use by women with a family history of breast cancer were not associated with an increased risk of the disease (3).
In a National Cancer Institute (NCI)-sponsored study published in 2003, researchers examined risk factors for breast cancer among women ages 20 to 34 compared with women ages 35 to 54. Women diagnosed with breast cancer were asked whether they had used OCs for more than 6 months before diagnosis and, if so, whether the most recent use had been within 5 years, 5 to 10 years, or more than 10 years. The results indicated that the risk was highest for women who used OCs within 5 years prior to diagnosis, particularly in the younger group (4).
Selected References
1. Burkman R, Schlesselman JJ, Zieman M. Safety concerns and health benefits associated with oral contraception. American Journal of Obstetrics and Gynecology 2004; 190(4 Suppl):S5–22.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: Collaborative reanalysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet 1996; 347:1713–1727.
3. Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. New England Journal of Medicine 2002; 346(26):2025–2032.
4. Althuis MD, Brogan DD, Coates RJ, et al. Breast cancers among very young premenopausal women (United States). Cancer Causes and Control 2003; 14(2):151–160.

The correlation between oral contraceptives and an increased risk in breast cancer is an area of concern to me. I have two young adult daughters...18 and 21 years.How do oral contraceptives affect breast cancer risk?
I myself was put on oral contraceptives when I was 16 years old and attending a co-ed boarding school. It was the school administration's way of combating scandal. During this chapter in my life (more like novella...) I discovered the hypothesis that the ingestion of oral contraceptives before age 20 may play into a women's increased likelihood of developing breast cancer later in adulthood. As with all of the "science" in the area of medicine and disease, it is another theory -- one with probably merit. There is always a consequence / impact / alteration when we introduce an agent (whether it be foreign or an amplification of one already naturally occurring) into our body chemistry. I am always leery, however, to accept such theories and studies. When it comes to medical theories and the funded study thereof, my first question is: "who underwrote the study, and what was their motivation (the "who" usually answers the latter query).
A woman’s risk of developing breast cancer depends on several factors, some of which are related to her natural hormones. Hormonal factors that increase the risk of breast cancer include conditions that may allow high levels of hormones to persist for long periods of time, such as beginning menstruation at an early age (before age 12), experiencing menopause at a late age (after age 55), having a first child after age 30, and not having children at all.
A 1996 analysis of worldwide epidemiologic data conducted by the Collaborative Group on Hormonal Factors in Breast Cancer found that women who were current or recent users of birth control pills had a slightly elevated risk of developing breast cancer. The risk was highest for women who started using OCs as teenagers. However, 10 or more years after women stopped using OCs, their risk of developing breast cancer returned to the same level as if they had never used birth control pills, regardless of family history of breast cancer, reproductive history, geographic area of residence, ethnic background, differences in study design, dose and type of hormone, or duration of use. In addition, breast cancers diagnosed in women after 10 or more years of not using OCs were less advanced than breast cancers diagnosed in women who had never used OCs. To conduct this analysis, the researchers examined the results of 54 studies. The analysis involved 53,297 women with breast cancer and 100,239 women without breast cancer. More than 200 researchers participated in this combined analysis of their original studies, which represented about 90 percent of the epidemiological studies throughout the world that had investigated the possible relationship between OCs and breast cancer (2).
The findings of the Women’s Contraceptive and Reproductive Experiences (Women’s CARE) study were in contrast to those described above. The Women’s CARE study examined the use of OCs as a risk factor for breast cancer in women ages 35 to 64. Researchers interviewed 4,575 women who were diagnosed with breast cancer between 1994 and 1998, and 4,682 women who did not have breast cancer. Investigators collected detailed information about the participants’ use of OCs, reproductive history, health, and family history. The results, which were published in 2002, indicated that current or former use of OCs did not significantly increase the risk of breast cancer. The findings were similar for white and black women. Factors such as longer periods of use, higher doses of estrogen, initiation of OC use before age 20, and OC use by women with a family history of breast cancer were not associated with an increased risk of the disease (3).
In a National Cancer Institute (NCI)-sponsored study published in 2003, researchers examined risk factors for breast cancer among women ages 20 to 34 compared with women ages 35 to 54. Women diagnosed with breast cancer were asked whether they had used OCs for more than 6 months before diagnosis and, if so, whether the most recent use had been within 5 years, 5 to 10 years, or more than 10 years. The results indicated that the risk was highest for women who used OCs within 5 years prior to diagnosis, particularly in the younger group (4).
Selected References
1. Burkman R, Schlesselman JJ, Zieman M. Safety concerns and health benefits associated with oral contraception. American Journal of Obstetrics and Gynecology 2004; 190(4 Suppl):S5–22.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: Collaborative reanalysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet 1996; 347:1713–1727.
3. Marchbanks PA, McDonald JA, Wilson HG, et al. Oral contraceptives and the risk of breast cancer. New England Journal of Medicine 2002; 346(26):2025–2032.
4. Althuis MD, Brogan DD, Coates RJ, et al. Breast cancers among very young premenopausal women (United States). Cancer Causes and Control 2003; 14(2):151–160.

Friday, February 4, 2011
Environmental Toxins and Cancer Risk
******

Heavy Metal Toxicity & Testing
In Maricopa County (Arizona) we are in the 90th to 100th percentile for cancer risk meaning our county is one of the most toxic counties in the United States - Scorecard*. Our biggest cancer risk comes from Cadmium a potent xenobiotic shown to do irreparable harm to nearly all organ systems. Heavy metals have been linked to a multitude of conditions including cancer, heart, kidney, infertility, neurological disease and much more.
Heavy metals are depurated through chelators including but not limited to DMPS, CaEDTA, and DMSA. Chelation is the only effective way to remove heavy metals due to the fact they are bioaccumulative and build up in the body with each exposure and have very long half lives.
*In Maricopa County . . . . . .from 1988 to 2002, total cancer risk scores have increased 681%.
Chemical Name / Cancer Risk Scores Pounds of benzene-equivalents
CADMIUM COMPOUNDS 6,500,000
CHROMIUM 62,000
TETRACHLOROETHYLENE 46,000
LEAD 18,000
LEAD COMPOUNDS 13,000
CHROMIUM COMPOUNDS 5,900
DICHLOROMETHANE 4,300
BENZENE 2,300
NICKEL 1,400
NICKEL COMPOUNDS 740
TRICHLOROETHYLENE 420
FORMALDEHYDE 220
METHYL TERT-BUTYL ETHER 82
Note: These rankings do not cover all chemical releases reported to TRI (Toxic Release Inventory) - they only include chemicals that possess risk scores. As a result of data gaps or modeling problems, not all TRI chemicals possess the information required to weight their mass release by toxicity and exposure potential. Dioxin compounds, for example, are not included in these rankings. TRI chemicals that lack risk scores should not be assumed to be safe.
http://scorecard.goodguide.com/env-releases/county.tcl?fips_county_code=04013#major_chemical_releases
Heavy Metal Toxicity & Testing
In Maricopa County (Arizona) we are in the 90th to 100th percentile for cancer risk meaning our county is one of the most toxic counties in the United States - Scorecard*. Our biggest cancer risk comes from Cadmium a potent xenobiotic shown to do irreparable harm to nearly all organ systems. Heavy metals have been linked to a multitude of conditions including cancer, heart, kidney, infertility, neurological disease and much more.
Heavy metals are depurated through chelators including but not limited to DMPS, CaEDTA, and DMSA. Chelation is the only effective way to remove heavy metals due to the fact they are bioaccumulative and build up in the body with each exposure and have very long half lives.
*In Maricopa County . . . . . .from 1988 to 2002, total cancer risk scores have increased 681%.
Chemical Name / Cancer Risk Scores Pounds of benzene-equivalents
CADMIUM COMPOUNDS 6,500,000
CHROMIUM 62,000
TETRACHLOROETHYLENE 46,000
LEAD 18,000
LEAD COMPOUNDS 13,000
CHROMIUM COMPOUNDS 5,900
DICHLOROMETHANE 4,300
BENZENE 2,300
NICKEL 1,400
NICKEL COMPOUNDS 740
TRICHLOROETHYLENE 420
FORMALDEHYDE 220
METHYL TERT-BUTYL ETHER 82
Note: These rankings do not cover all chemical releases reported to TRI (Toxic Release Inventory) - they only include chemicals that possess risk scores. As a result of data gaps or modeling problems, not all TRI chemicals possess the information required to weight their mass release by toxicity and exposure potential. Dioxin compounds, for example, are not included in these rankings. TRI chemicals that lack risk scores should not be assumed to be safe.
http://scorecard.goodguide.com/env-releases/county.tcl?fips_county_code=04013#major_chemical_releases
Thursday, February 3, 2011
All the Good Advice
******
 What do all of life's milestones have in common? E.g., marriage, college choices, pregnancy, parenthood, cancer? It would appear that with each there is no shortage of "good advice" from well-meaning sources. Even 18 months into this journey, the "good advice" keeps cropping up. A few of these tidbits are definitely worth serious look and consideration. Others...well, let's just say they raise both questions and eyebrows. I share some of the most memorable. Any insight regarding the following would be appreciated, not only for my edification but also for the entertainment value:
What do all of life's milestones have in common? E.g., marriage, college choices, pregnancy, parenthood, cancer? It would appear that with each there is no shortage of "good advice" from well-meaning sources. Even 18 months into this journey, the "good advice" keeps cropping up. A few of these tidbits are definitely worth serious look and consideration. Others...well, let's just say they raise both questions and eyebrows. I share some of the most memorable. Any insight regarding the following would be appreciated, not only for my edification but also for the entertainment value:
You should be consuming only an alkaline diet -- including water, to combat acidity.Acidity in the body gives a fertile environment for cancer cells to attach and proliferate.
You should not consume cooked spinach or blueberries.
You should never wear anything but cotton bras. Synthetic bras irritate the breast tissue and is associated with the recurrence of breast cancer.
You should adopt a vegan diet - being an organic, predominate vegetarian is not sufficient.
You should not drink well water.
You should not drink tap water.
You should not drink bottled water.
You should make sure to double your intake of water.
You should not eat any meat that has been grilled or pan-seared.
You should not eat any red meat whatsoever.
You should not any type of animal protein what-so-ever, including seafood.
Don't consume soy-based foods -- soy is a natural estrogen and increases breast cancer risk.
You should be doing an infrared sauna at least 4x per week.
You should not wear bras with underwire. Underwire increases the risk of breast cancer.
You should be consuming 3000-10,000 IU of Vitamin D daily. Lack of Vitamin D is a factor in breast cancer.
You should not be taking any Vitamin D supplements - high doses of Vitamin D can lead to toxicity.
You should be having your iodine levels checked every six weeks.
You should be having your Vitamin D levels checked every six weeks.
You should be tested for heavy metals.
You should be drinking Yerba Mate tea daily for its antioxidants.
You should be drinking Green Tea daily for its antioxidants.
You should be getting weekly massages to help detox your body.
You should not be having massages while you do bodywork.
and my three favs...
You should be doing a coffee colonic weekly. The properties in coffee can combat the acidity in your digestive system.
You should be doing a candida colonic bi-weekly - to remove yeast from your intestines. The presence of yeast undermines your immune system -- which can increase your susceptibility to a recurrence.
You should be doing a colon hydrotherapy weekly to detox your system.

You should be consuming only an alkaline diet -- including water, to combat acidity.Acidity in the body gives a fertile environment for cancer cells to attach and proliferate.
You should not consume cooked spinach or blueberries.
You should never wear anything but cotton bras. Synthetic bras irritate the breast tissue and is associated with the recurrence of breast cancer.
You should adopt a vegan diet - being an organic, predominate vegetarian is not sufficient.
You should not drink well water.
You should not drink tap water.
You should not drink bottled water.
You should make sure to double your intake of water.
You should not eat any meat that has been grilled or pan-seared.
You should not eat any red meat whatsoever.
You should not any type of animal protein what-so-ever, including seafood.
Don't consume soy-based foods -- soy is a natural estrogen and increases breast cancer risk.
You should be doing an infrared sauna at least 4x per week.
You should not wear bras with underwire. Underwire increases the risk of breast cancer.
You should be consuming 3000-10,000 IU of Vitamin D daily. Lack of Vitamin D is a factor in breast cancer.
You should not be taking any Vitamin D supplements - high doses of Vitamin D can lead to toxicity.
You should be having your iodine levels checked every six weeks.
You should be having your Vitamin D levels checked every six weeks.
You should be tested for heavy metals.
You should be drinking Yerba Mate tea daily for its antioxidants.
You should be drinking Green Tea daily for its antioxidants.
You should be getting weekly massages to help detox your body.
You should not be having massages while you do bodywork.
and my three favs...
You should be doing a coffee colonic weekly. The properties in coffee can combat the acidity in your digestive system.
You should be doing a candida colonic bi-weekly - to remove yeast from your intestines. The presence of yeast undermines your immune system -- which can increase your susceptibility to a recurrence.
You should be doing a colon hydrotherapy weekly to detox your system.
Subscribe to:
Posts (Atom)